While the eyes of the world were concentrated on Europe, a new strain of influenza, unlike any seen before, was born. Within five months, the new strain had circled the globe and further mutated itself to become the powerful killer it was.
When influenza first appeared in America in March of 1918, the nation paid little heed to it. The Russians had just withdrawn from World War I and Germany was moving division after division to the Western Front in order to gain numerical superiority over the opposing British and French troops. On March 21, the Germans launched a huge offensive, overrunning large areas of France in just three weeks. As a reply to urgent appeals from the Allies, America sent a total of 202,000 troops to France. America began the largest mobilization in its history. Consequently, the Country's lack of attention to the relatively mild first wave of the Great Pandemic is not surprising. (1) But, while few took notice, something new and deadly was seeding itself in the throats and lungs of Americans that would bury more human beings than the War. (2)
Indeed, the war effort, and not influenza, occupied most people's minds that spring. This lack of attention was partly due to the disease itself. Pneumonic complications were rare and deaths were even more infrequent. Influenza seemed no worse than any other type of respiratory infection common to the early spring. (3) Quite possibly, many doctors mistook many cases of influenza as common colds, making the presence of influenza even less noticeable.
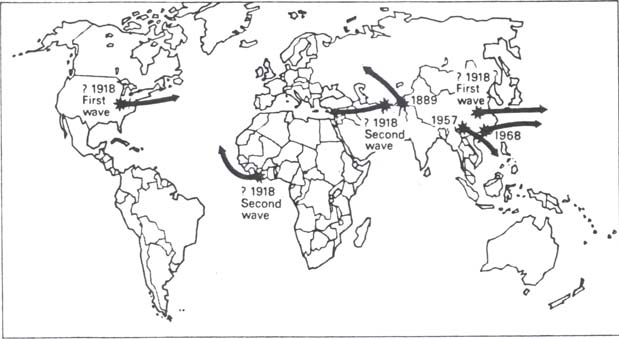
Figure 2 — The Starting Points of the Last Four Pandemics (4)
{kind=link}
The first wave probably began in the United States and was brought to Europe by the American Expeditionary Force (AEF). Another possible starting point was China (see Figure 2) where influenza was reported in early March. The Japanese Navy also reported cases of the disease at about the same time, however, no reliable documentary evidence exists to support this. An interesting point to note is that China was the point of origin for the pandemics of 1889, 1957, and 1968. The interior of Eastern Asia is apparently the birthplace for influenza pandemics, and as the other three major pandemics of the last 100 years began there, it would seem logical that the 1918 pandemic also started there. However, if evidence from qualified sources is required to conclude the starting point of the epidemic, then the United States must be seen as the origin of the first wave. (5)
By the end of March, a mild form of influenza had passed through many of the states east of the Mississippi River, and a few west of the River. The disease first appeared in France in the base ports of the AEF the following month, and reached the front lines at the end of the month. The disease crossed to the German front at the beginning of May, and then began its journey through Eastern and Central Europe. (6)
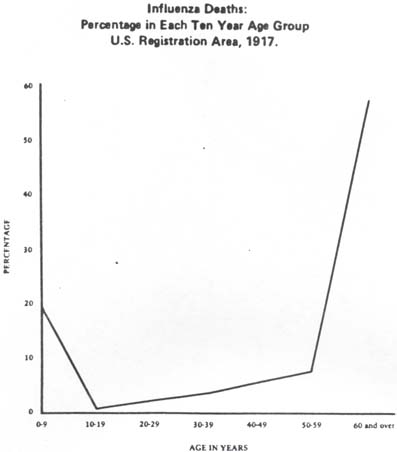
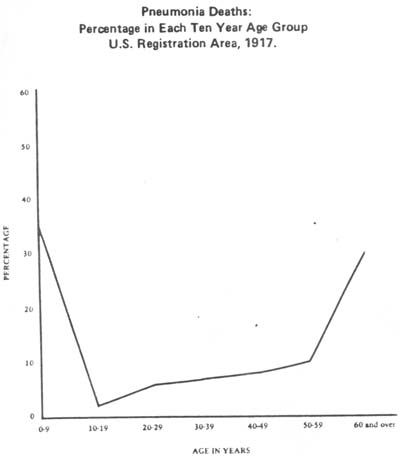
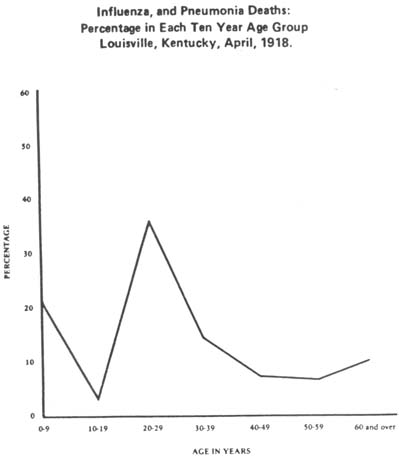
At the time, influenza was not a reportable disease, creating difficulties in obtaining a clear picture of the Spring epidemic. Death certificates from the period are not helpful either; most physicians attributed deaths to uncomplicated pneumonia. In an age before penicillin and sulfa drugs, pneumonia was not an uncommon way to die, especially in the winter or early spring. (7) The spring wave was mild when compared to the second wave of the fall. Diagnostic confusion between influenza and other common respiratory infections undoubtedly led to the unclear understanding of the spring wave. Nevertheless, the spring epidemic did have two distinguishing features which were ominous signs of what laid ahead. In post-mortems of the victims of the spring wave, pathologists found something new in the victim's lungs: a wipespread hemorrhagic and edematous (abnormal excess buildup of fluid) process never before seen with influenza. The second significant feature was the suprising age of the victims. Both influenza and pneumonia usually kill the age extremes of the population, the very young or very old. On a graph, this would appear as a rough "U." (See Figure 3, influenza deaths, and Figure 4, pneumonia deaths) This mortality pattern has remained relatively constant. A similar graph for the 1918 spring wave and later waves of the pandemic revealed the shape of the curve as a crude "W" with the peak in the middle, "where both science and common sense declare it should not be." (8) (See Figure 5, p. 17)
{kind=link}
{kind=link}
{kind=link}
Figure 3: Influenza Deaths: Percentage in Each Ten Year Age Group, U. S. Registration Area, 1917. (9)
Figure 4: Pneumonia Deaths: Percentage in Each Ten Year Age Group, U. S. Registration Area, 1917. (10)
Figure 5: Influenza and Pneumonia Deaths: Percentage in Each Ten Year Age Group, Louisville, Kentucky, April, 1918. (11)
These data suggest that people in the United States between the ages of twenty and forty, in the prime of their lives, were dying more than the more vulnerable young and old.
The Bureau of the Census has issued a report based on the mortality in Indiana, Kansas and Philadelpha for the period September 1st to December 31st. It shows that the highest rate occurred in the age period from 30 to 34 years, with the period from 25 to 29 years second. Of all the deaths tabulated, more than half occur — this age group represents only 33 percent of the total population concerned. (12)
This pattern of mortality was not confined to the United States, but found throughout the world. Apparently, the older Americans, who had lived through a previous influenza epidemic of 1889-90, had developed an immunity to the disease.
In the United States, recent immigrants to this country seem to generally have a higher mortality rate than native born Americans. The bulk of these immigrants, mostly Italians, Russians, and Poles, were between the ages of twenty and forty. Obviously, they were equally as susceptible to influenza as their native born counterparts. The reason for the immigrants higher mortality appears to have been their living conditions. Since influenza is most easily passed in crowded conditions, the congested tenements where most immigrants lived provided the atmosphere for higher mortality. (13)
The studies of both Winslow and Rogers, and Vaughan supported the conclusion that the living conditions of the immigrants contributed to their higher death rates. Winslow and Rogers showed that in Connecticut, the mortality of native-born Americans of Irish, English and German stock was much lower than the mortality for Italians, Russians and Poles. (14) In his study of the effects of influenza in the Greater Boston area, Vaughan found that the Italian and Jewish (made-up of mostly Russians and Poles) tenements were the most severely struck, while the Irish, who were second or third generation native-born American, and whose living conditions were much better than the Italians and Jews, not nearly as affected. (15)
In the four months following influenza's initial appearance in the United States (April to July), the disease had circled the globe and was raised from epidemic to pandemic status. Although the first wave was considered mild, it probably killed tens of thousands world-wide, but the next wave would kill millions. In America, a surprising absence of influenza marked the summer of 1918, a calm before the storm. The disease, however, seemed to have America surrounded. Early July saw epidemics erupt in Cuba, Puerto Rico and Panama. Chinese and Japanese shipping brought the disease to the Hawaiian Islands. With the exception of a mild outbreak at Fort Morgan, Alabama, influenza seemed unable to penetrate the country's coast.
This absence of influenza in America during July and August was probably due to the fact that it was the summer time. (16) Influenza epidemics peak in the Northern Hemisphere in January and February, but epidemics frequently begin in November or December. There seem to be two major factors that make influenza a winter disease. The most important of these is that people spend more time indoors during the cold months of the year. The crowding of people in poorly ventilated buildings facilitates the transmission because the spread of influenza is highly dependant on the population density of a community. The other factor that helps influenza spread is the increased frequency of sneezing and coughing due to more colds during the winter. Unlike the Northern Hemisphere, the tropics do not have a specific flu season. Summer and early fall outbreaks of influenza, such as the second wave, that occur in the Northern Hemisphere are generally attributed to the introduction of a new pandemic strain. While America was enjoying its brief respite, the virus was working its way through millions of people across Asia, Africa and Europe. Somewhere along the line, the virus's genetic character changed. As noted by Vaughan, "During its course through Europe influenza had developed a greatly heightened virulence". (17)
Chapter II Footnotes
- Alfred Crosby, Epidemic and Peace, 1918, 1976, p.18.
- Ibid., p. 21.
- June Osborn, History, Science and Politics: Influenza in America, 1977, p. 6.
- William Beveridge, Influenza, The Last Great Plague, 1977, p. 41.
- Ibid., p. 42.
- Warren Vaughan, Influenza: An Epidemiological Study, July, 1923, pp. 65-68.
- Crosby, p. 18.
- Ibid., p. 21.
- Ibid., p. 22.
- Ibid., p. 23.
- Ibid., p. 24.
- Vaughan, p. 168.
- Robert Katz, "Influenza 1918-1919: A Study in Mortality," Bulletin of the History of Medicine, Fall 1974, pp. 416-422.
- C. E. Winslow, et al., "Statistics of the 1918 Epidemic of Influenza in Connecticut," Journal of Infectious Disease, 1920, Vol. 26, pp. 175-215.
- Vaughan, pp. 129-132, 142-143.
- The following discussion is based on Beveridge, pp. 44-48.
- Vaughan, p. 68.